Ulcerative Colitis: The Mucosal Siege That Never Ends
Ulcerative colitis confines its destruction to the inner lining of the large intestine, but the sustained mucosal inflammation produces continuous pain, bleeding, and over decades, significantly elevated colorectal cancer risk. The disease begins at the rectum and spreads proximally.
What is happening in the body
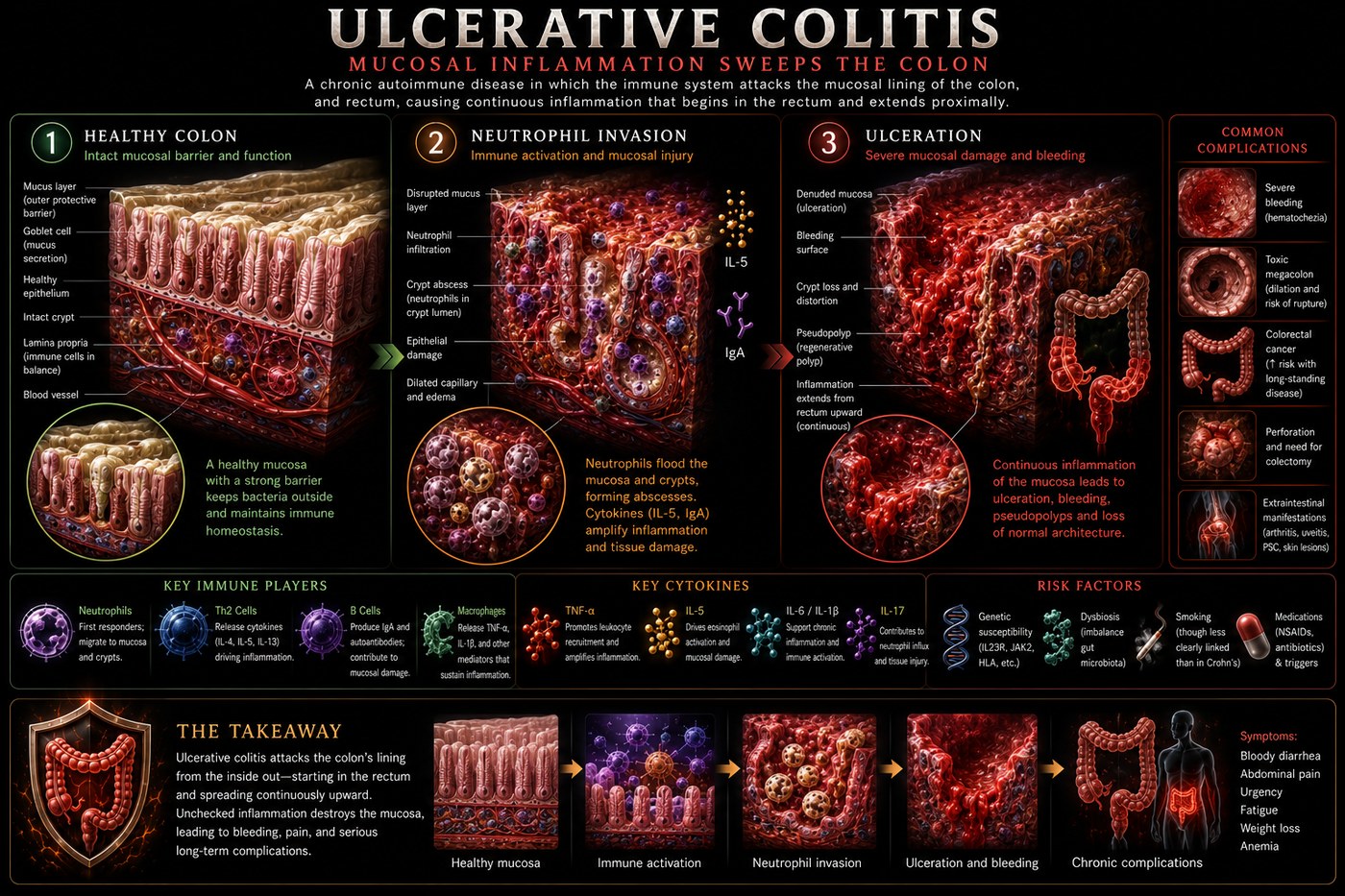
Ulcerative colitis is a disease of the colon's mucosal surface. Unlike Crohn's disease, which can strike anywhere in the gastrointestinal tract and penetrates all layers of the gut wall, UC is confined to the mucosa and submucosa of the large intestine, always beginning at the rectum and extending proximally in a continuous, uninterrupted pattern. Proctitis affects only the rectum; left-sided colitis extends to the splenic flexure; pancolitis reaches the caecum.
The initiating event appears to be a breakdown in epithelial barrier function in genetically susceptible individuals. Luminal bacteria and bacterial products cross the mucosal barrier and trigger an exaggerated innate immune response. Neutrophils — the first responders of innate immunity — flood the lamina propria and invade the crypts of Lieberkühn, the test-tube-shaped glands that run perpendicular through the colonic mucosa. When neutrophils pack a crypt completely, the result is a crypt abscess, visible on colonoscopy biopsy.
Crypt abscesses rupture and coalesce into mucosal ulcers — raw, bleeding patches that produce the cardinal symptoms of bloody diarrhoea. The chronic inflammation progressively depletes goblet cells (which produce the protective mucous layer) and distorts the normal crypt architecture, producing the crypt branching and foreshortening visible on histology.
The symptoms this produces
- Bloody diarrhoea — the defining symptom
- Urgency and tenesmus (painful urge to defecate without result)
- Cramping lower abdominal pain, usually left-sided
- Mucus in stool
- Fatigue and anaemia from chronic blood loss
- Toxic megacolon in severe cases (life-threatening)
- Colorectal cancer risk increasing significantly after 8–10 years of pancolitis
How this fits the autoimmune pattern
UC shares the upstream mechanism of increased intestinal permeability with Crohn's, but the immune response targets surface antigens rather than penetrating deeper. Dysbiosis — reduced Faecalibacterium prausnitzii, overgrowth of Fusobacterium and adherent-invasive E. coli — is consistently documented in UC and precedes flares. The disrupted microbiome reduces short-chain fatty acid (SCFA) production, particularly butyrate, which is the primary fuel source for colonocytes and the key regulator of colonic mucosal integrity and immune tolerance.
What the clinical data shows
Elimination of fermentable fibre and plant compounds on the PKD removes the substrates driving pathological dysbiosis. Several UC patients in Paleomedicina's case series achieved mucosal healing confirmed by colonoscopy — the gold standard endpoint — while on PKD, reducing or eliminating 5-aminosalicylate and corticosteroid dependence. The mechanism is restoration of colonocyte energy metabolism through ketone bodies (which partly substitute for the butyrate deficit) and elimination of the permeability-promoting dietary factors that perpetuate the mucosal injury cycle.
A life with this condition — Stories
Elena, 29. She knew something was wrong the fourth time she needed the bathroom in three hours at work. The bleeding had started three weeks earlier — intermittent at first, then constant. By the time she saw her GP she was anaemic. The colonoscopy showed continuous inflammation from rectum to splenic flexure, the surface raw and friable. She was started on mesalazine and told to monitor for worsening. For the next decade the question was not whether she would flare, but when — and what the increasing cumulative burden of inflammation would mean for her cancer risk.
Jason, 42. His severe flare came without warning after a course of antibiotics for a dental abscess. He was admitted with eight bloody stools per day, a CRP of 210, and a heart rate of 112. The gastroenterologist said the word "colectomy" in the first conversation, which was the first time Jason understood that this disease could end with his colon removed. IV steroids brought him back from the edge of surgery that admission, but his gastroenterologist told him plainly: one more severe flare at this level and the decision would be made for him. He started a biologic the week he was discharged.
Maria, 57. She had lived with pancolitis for 22 years, learned to manage it, and regarded it as controlled. What her gastroenterologist found on her surveillance colonoscopy was not. A flat lesion in the transverse colon — low-grade dysplasia, technically not cancer, but in the context of 22 years of mucosal inflammation a serious warning. She was referred for colectomy. The surgery she had spent two decades avoiding became necessary not because of a flare but because of the invisible accumulation of damage that decades of inflammation had quietly laid down.
Transcript witness — Dr. Anthony Chaffee podcast. A gastric surgeon describing his moment of realisation: "I can remember the moment I learned that autoimmune diseases are actually reversible. I said, 'Wild. Why? Why did nobody tell me that? How come I don't know that? How come you go to the textbook and it doesn't have anything that is cure?' I cut out people's colons because their ulcerative colitis had boring big holes and ulcers in it. They died. And you're telling me if I would have changed the freaking menu? That's the answer. That is a guilt I will hold for the rest of my life."
Hannah, 34. She had been hospitalised twice with toxic megacolon — the rare, life-threatening complication of severe UC where the colon loses its muscle tone and balloons. Twice she had been within hours of a colectomy, and twice IV ciclosporin had pulled her back from surgery. Her gastroenterologist told her that a third episode would almost certainly end with surgery. She started an exclusion diet between hospitalisations, not from confidence but from the understanding that the trajectory she was on had a clear destination, and she needed to try something different before she arrived there.
Patrick, 51. His UC had been in remission for eight years when he retired and found, within three months, that the stress reduction of retirement coincided with the best bloods he had recorded in a decade. His gastroenterologist noted that psychosocial stress is a consistent flare trigger in UC through HPA axis activation of intestinal mast cells. Patrick had been managing his disease well on medication. He had not known that his job had been managing it badly in parallel. The retirement was the dietary and lifestyle intervention his disease had been waiting for.
Zara, 26. She was vegetarian and her gastroenterologist supported this, emphasising the importance of fibre for gut health. She had four flares in eighteen months. She eventually tried — against everything she had been told — removing fibre from her diet. The flare she was in at the time resolved within two weeks. Her calprotectin, which had been over 2000, dropped below 100 within three months. She came back to her gastroenterologist with the results. He reviewed them in silence. He said: "This is not what the guidelines say. But those are your numbers."