Ankylosing Spondylitis: When the Spine Fuses Itself Shut
Ankylosing spondylitis targets the sacroiliac joints and spine with a unique perversity: instead of merely destroying joints, it replaces them with new bone. The final outcome, without treatment, is a fused, immobile spine — the "bamboo spine" of advanced disease.
What is happening in the body
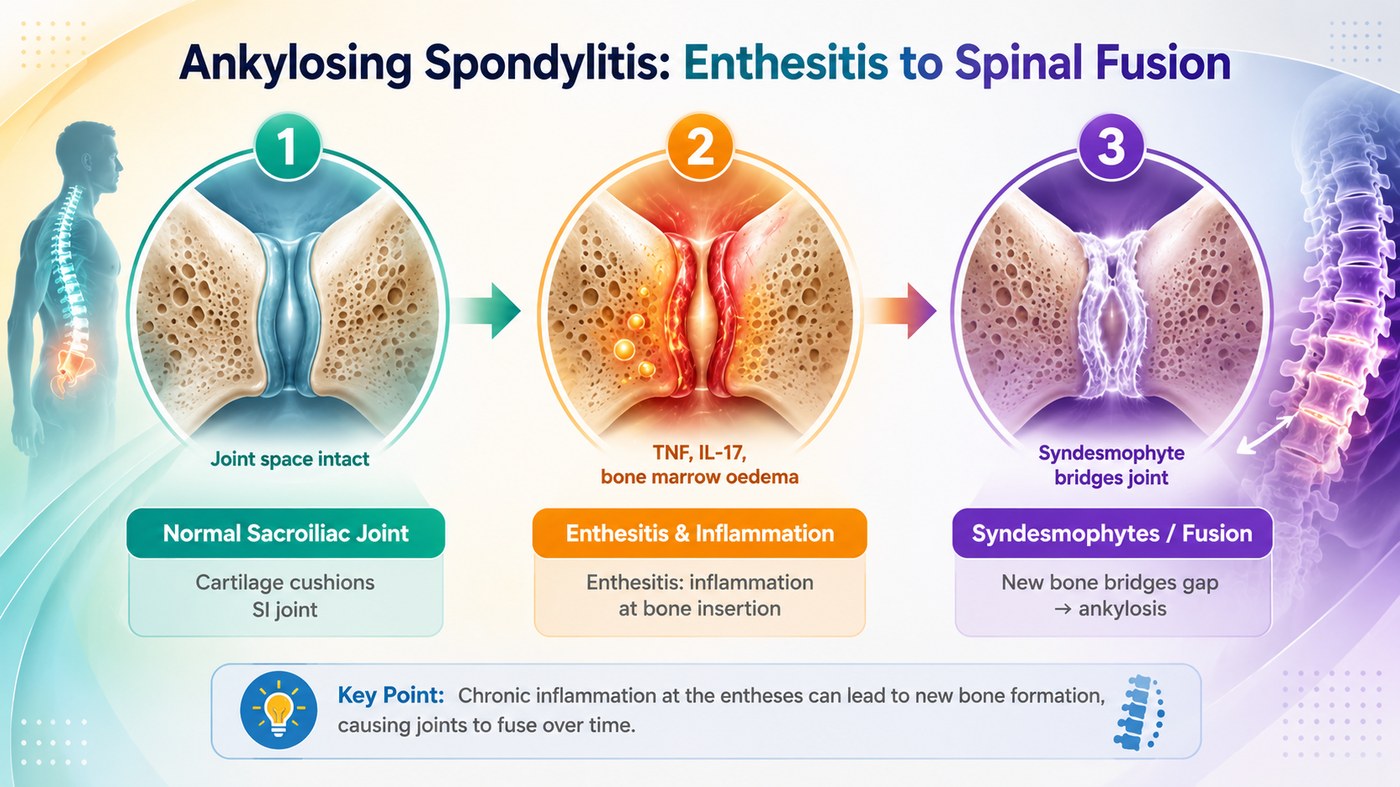
Ankylosing spondylitis begins at the entheses — the sites where ligaments, tendons, and joint capsules attach to bone. The sacroiliac joints are the initial target in over 90% of cases, producing the characteristic buttock pain and morning stiffness that may precede diagnosis by years. The entheseal inflammation (enthesitis) is driven by IL-17, IL-23, and TNF-alpha, produced by innate-like lymphocytes (ILC3 cells and MAIT cells) that reside at entheseal sites and respond to microbial signals from the gut.
What distinguishes AS from all other inflammatory arthritides is the osteoproliferative response. Instead of bone erosion (as in RA), AS triggers new bone formation. The entheseal inflammation stimulates osteoblast activity, and the repair response lays down new bone at the inflamed insertion sites. In the spine, this produces syndesmophytes — bony bridges growing from the vertebral body edges — that progressively span the disc spaces. Over decades, adjacent vertebrae fuse completely, producing the "bamboo spine" on plain X-ray: a single calcified column with no disc spaces visible.
The symptoms this produces
- Inflammatory back pain: worse in the morning, improves with exercise, not rest
- Sacroiliac joint pain — buttock pain alternating sides
- Progressive loss of spinal mobility — reduced lumbar flexion, chest expansion
- Fatigue
- Anterior uveitis — eye inflammation, the most common extra-articular feature
- Peripheral arthritis (hip, shoulder in more severe cases)
- Increased fracture risk from spinal rigidity
How this fits the autoimmune pattern
AS is the autoimmune condition most directly linked to gut inflammation. Over 60% of AS patients have subclinical gut inflammation on ileocolonoscopy, and 5–10% develop clinically manifest IBD. The Klebsiella pneumoniae hypothesis proposes that pullulanase — a starch-degrading enzyme produced by Klebsiella — mimics HLA-B27 (present in 90% of AS patients) and triggers the inflammatory response. Starch feeds Klebsiella selectively, and a low-starch diet has been shown in clinical studies to reduce Klebsiella counts, IgA anti-Klebsiella antibodies, and disease activity in AS patients.
What the clinical data shows
The low-starch diet was pioneered specifically for AS by Alan Ebringer at King's College London, based on the Klebsiella hypothesis. Clinical trials demonstrated significant reduction in acute-phase reactants and disease activity scores. The PKD, which is zero-starch by design, represents the maximally effective implementation of this principle. Paleomedicina patients with AS have shown MRI improvement in sacroiliac joint inflammation and reduction in BASDAI (disease activity) scores, with some achieving complete clinical remission.
A life with this condition — Stories
Marcus, 26. His GP diagnosed a muscle strain and recommended rest. But rest made it worse — he was stiffest after long nights in bed, loosening up only after an hour of movement. He described his mornings as "rusting open." Three years later, an X-ray showed the first syndesmophytes bridging his lower lumbar vertebrae. The MRI of his sacroiliac joints lit up with bone marrow oedema — enthesitis. His immune system was attacking the ligament insertion points, and his repair response was building new bone in their place, slowly fusing his spine from the bottom up. His rheumatologist told him that without a DMARD he would likely have a bamboo spine by 50.
Nadia, 24. Her AS took four years to diagnose partly because she was a young woman. Ankylosing spondylitis is still widely perceived as a disease of young men; women with axial spondyloarthritis tend to have more peripheral joint involvement and less classical sacroiliac changes on plain X-ray, making the diagnosis less obvious. Her rheumatologist eventually found her HLA-B27 positive and her MRI showed sacroiliac oedema that plain X-ray had missed entirely. She had been told repeatedly that her pain was related to her menstrual cycle. It was not.
Richard, 34. His AS was found through his eye, not his spine. He had his third episode of anterior uveitis — a sudden, painful red eye with sensitivity to light — when his ophthalmologist asked if he had back stiffness in the mornings. He did, but had not mentioned it because he thought it was unrelated. The rheumatology referral produced a positive HLA-B27, an MRI showing established sacroiliitis, and a diagnosis of ankylosing spondylitis. The eye inflammation had been his body's recurring announcement of a spinal disease he had been living with unknowingly for years.
Transcript witness — zerocarb community. A woman who moved to Germany and developed AS: "About 30 years ago I moved to Germany and got into the culture — cake every day, breaded schnitzel, German beer. My wheat uptake went up significantly. Before I knew it I had a myriad of illnesses. The first autoimmune diagnosis was ankylosing spondylitis. With me it came out in my eyes — I kept having inflammation of the iris. They tested me and found I was HLA-B27 positive. The connection between the wheat, the gut, and the spine took me years to make, because nobody made it for me."
Transcript witness — zerocarb community. A man with AS reflecting on carnivore: "I have been diagnosed with ankylosing spondylitis. They call it bamboo spine. I have always thought I was really stiff — I always worked out and pushed through it. Since going carnivore, the stiffness is different. I do not know how to explain it except that it is less constant. The eczema I also have has stabilised. The AS and the eczema and the ADHD — I always thought these were separate things. I am not so sure anymore."
Omar, 31. He was HLA-B27 positive from a test ordered after his older brother was diagnosed with AS. He had no symptoms at the time. For three years he monitored, knowing the risk. The sacroiliac pain arrived when he was 30, six months after he had gained significant weight and changed jobs to a desk-based role. His rheumatologist started a NSAID and explained that the disease might have been triggered by the change in activity level and the weight gain, which increased mechanical load at the entheses. The genetics had been there all along. The trigger had waited for the right conditions.
Francesca, 38. Her AS responded well to a TNF-alpha inhibitor and she had been in clinical remission for four years when she decided to try pregnancy. Biologics carry fetal risks and are typically stopped in the second trimester; her rheumatologist and obstetrician co-managed the switch to sulfasalazine, which is safer in pregnancy but less effective. She flared at 28 weeks. The flare was managed with short-course corticosteroids. Her baby was healthy. The postpartum period brought a further flare as immune tolerance mechanisms lifted. She restarted her biologic at eight weeks postpartum. Managing AS through pregnancy required more medicine, more monitoring, and more decisions than she had anticipated when she first read that the disease was "compatible with normal life."
Dev, 43. His bamboo spine on plain X-ray was discovered incidentally during a chest X-ray for an unrelated respiratory matter. He had not been diagnosed with AS. He had been stiff, he had had back pain for years, and he had managed both with ibuprofen and a physiotherapist who told him his core was weak. The radiologist's report used the words "advanced ankylosing spondylitis with bridging syndesmophytes at all lumbar levels." He brought the report to his GP, who referred him to rheumatology. He was told that his disease was too advanced for the biologics that might have slowed it in earlier stages to make a significant structural difference. The X-ray had found the final chapter of a story nobody had been watching.