Myasthenia Gravis: When Signals Can No Longer Reach the Muscles
Myasthenia gravis is caused by antibodies that block acetylcholine receptors at the neuromuscular junction. The nerve fires normally, but the signal cannot be received by the muscle. The hallmark is fatigable weakness — muscles that work at rest but fail progressively with use.
What is happening in the body
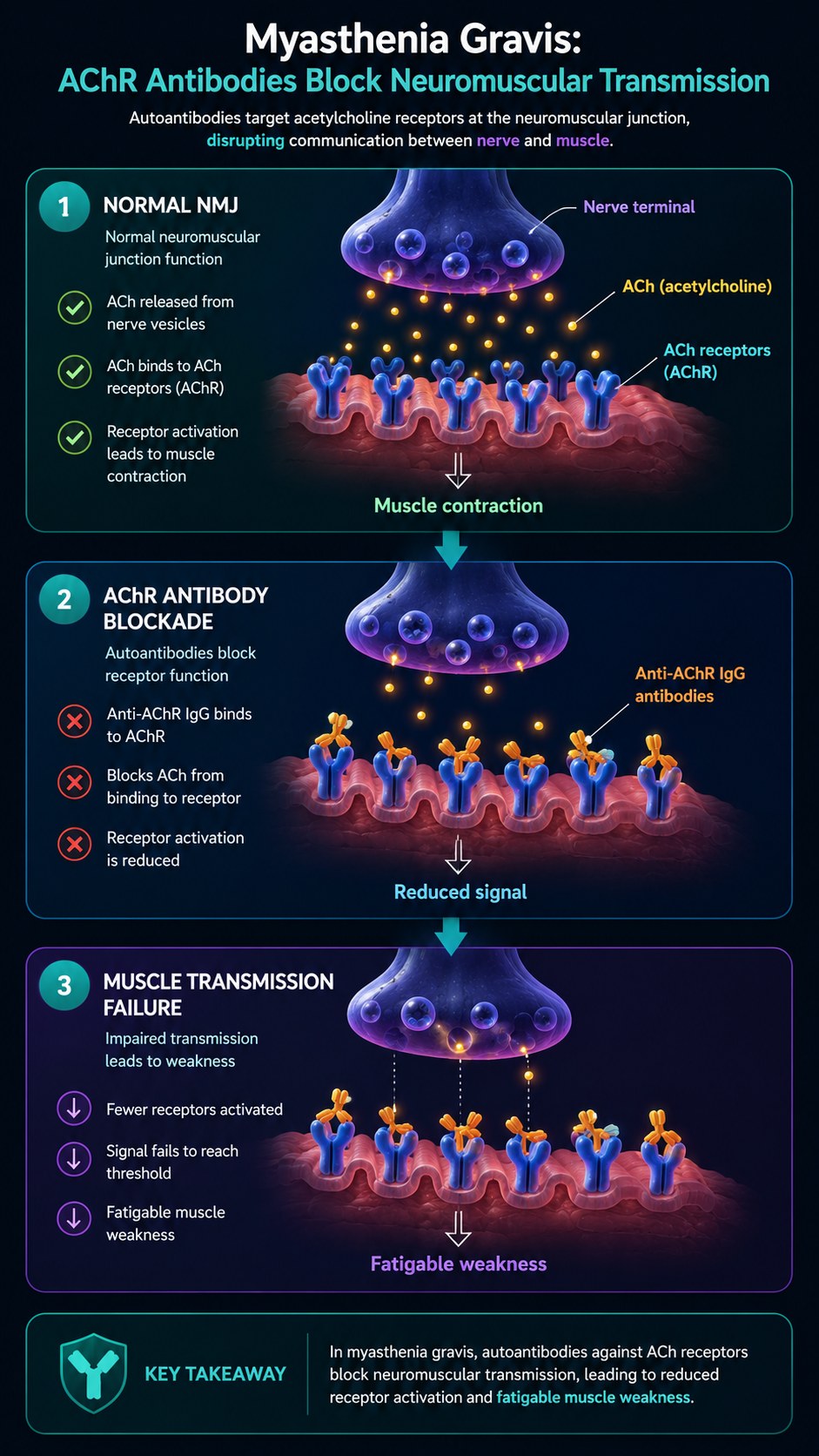
Voluntary muscle contraction requires a reliable chain of communication from nerve to muscle. At the neuromuscular junction (NMJ), a motor nerve terminal releases acetylcholine (ACh) vesicles into the synaptic cleft when an action potential arrives. ACh diffuses across the cleft and binds to acetylcholine receptors (AChR) on the muscle end-plate, triggering the ion flux that initiates muscle contraction. In myasthenia gravis, IgG antibodies directed against the AChR's alpha subunit — the ACh binding site — occupy and block those receptors. They also activate complement at the NMJ, degrading the receptor density of the post-synaptic membrane over time.
The clinical hallmark — fatigable weakness — reflects the physiological consequence of reduced receptor density. At rest, enough receptors remain unblocked for adequate transmission. With repeated use, the vesicle release per stimulus declines (normal synaptic fatigue), but with a reduced receptor density there is no margin to compensate. Transmission fails progressively within the same muscle contraction sequence. Resting restores some capacity, explaining why MG patients are weakest at the end of a task and strongest after sleep.
The symptoms this produces
- Ptosis — drooping eyelids, typically asymmetric and worse at day's end
- Diplopia — double vision from asymmetric extraocular muscle involvement
- Dysarthria and dysphagia — slurred speech, difficulty swallowing
- Proximal limb weakness — difficulty raising arms or climbing stairs
- Myasthenic crisis: respiratory muscle failure requiring ventilation
- Symptoms worsen with heat, illness, and exertion
How this fits the autoimmune pattern
The AChR-specific B cells that produce the pathogenic IgG require thymus-based T cell help — which is why the thymus is abnormal in 75% of AChR-positive MG patients (thymoma in 10%, thymic hyperplasia in 65%). Thymectomy is the only curative intervention and confirms the thymic origin of the autoimmune breach. The gut-thymus axis and the shared mechanisms of gut-driven autoimmunity connect MG to the same upstream permeability terrain. IgG anti-AChR titres correlate with systemic inflammatory markers and fall when the systemic immune burden is reduced.
What the clinical data shows
MG is less frequently documented in the PKD literature, reflecting the rarer presentation of thymoma-associated cases. However, ocular MG — the limited form affecting only eye muscles — and generalised MG in patients without thymoma have shown improvement in disease activity scores on anti-inflammatory diets. The primary therapeutic value of dietary intervention is reduction of the systemic inflammatory drive that maintains AChR-directed B cell activity, potentially reducing antibody titres and disease severity over time.
A life with this condition — Stories
Fiona, 41. She first noticed her left eyelid drooping on a photograph. Within a week she was wearing an eye patch to drive. Her neurologist performed an edrophonium test and watched her eyelid lift completely for ninety seconds before falling again — a brief, chemical reversal of the antibody blockade. The mechanism he described was almost offensively mechanical: antibodies sitting in the docking ports of her muscle receptors, blocking the acetylcholine trying to land. Her nerves were firing. The messages were arriving. There was simply nowhere to deliver them. By evening every day she had used up whatever the morning had given her.
George, 68. His MG diagnosis came via a CT scan ordered for an unrelated cough, which found a thymoma — a tumour of the thymus gland that is present in 10% of MG patients. He had been having mild swallowing difficulties for months that he had attributed to reflux. The thymoma was removed surgically; the myasthenia gravis, which the tumour had been generating, was confirmed by anti-AChR antibody testing during his admission. His surgery was successful, and his antibody titres declined over the following year. Thymectomy is the only intervention that addresses the source of AChR-directed B cell activation rather than managing its downstream effects.
Emma, 24. She spent eight months being investigated for a functional neurological disorder before a neurologist thought to test acetylcholine receptor antibodies. Her drooping eyelid had been attributed to stress; her swallowing difficulty had been attributed to anxiety. She had been referred for psychotherapy. Her anti-AChR titre came back at 18 nmol/L — markedly elevated. She started pyridostigmine that week. The eyelid lift was visible within an hour of the first dose. She had been offered an explanation for a physical disease that reduced its cause to her psychology. The antibody test ended eight months of that.
Transcript witness — metabolicmind podcast. Mary, describing her experience with MG and ketogenic diet: "I started having symptoms again of my illness. I had been diagnosed with myasthenia gravis and I was actually using a wheelchair for quite a few years back in 2012. I started to feel like I was getting sick again and so I started looking for new dietary changes to make. I found out about the ketogenic diet, started the protocol, and I started to improve. I have not returned to the wheelchair. I want other people with MG to know that I looked, and I found something, and it worked."
Clem, 66. His thymectomy had been successful in removing the thymoma, and his neurologist had told him that anti-AChR titres typically decline after thymectomy — sometimes slowly, sometimes dramatically. His titres declined slowly. Eighteen months after surgery, his MG was better but not gone. He was still on pyridostigmine and had added prednisolone for the months when the disease was most active. His neurologist told him that some patients achieve complete stable remission after thymectomy and some do not; the thymus generates the disease, but the B cell memory that maintains it can persist independently. He was in the second category, learning to be patient with an outcome that was better, but not finished.
Ingrid, 37. She managed her MG through two pregnancies — a process her neurologist described as "high-risk but manageable." MG can worsen or improve unpredictably in pregnancy; her first pregnancy improved her disease, her second worsened it. Her second baby was born with neonatal MG — a transient condition in which maternal anti-AChR antibodies cross the placenta and cause temporary muscle weakness in the newborn. Her baby required respiratory support for eight days in the NICU before the antibodies cleared and strength returned. Her neurologist had warned her this could happen; the warning had not made those eight days easier.
Transcript witness — Dr. Anthony Chaffee podcast. On the thymic origin of MG and dietary modulation: "Myasthenia gravis is one of the most mechanistically clear autoimmune conditions — the thymus generates the B cells that produce AChR antibodies, and thymectomy is the only intervention that addresses the source. But the gut-thymus axis is real: the same systemic immune activation that primes autoreactive B cells in other autoimmune conditions operates here too. Reducing the systemic inflammatory load through diet reduces the peripheral activation that maintains AChR-directed antibody production. It does not replace thymectomy. But it may shift the trajectory."
Lola, 22. She developed MG as a complication of checkpoint inhibitor therapy — the immunotherapy she was receiving for a stage 3 melanoma. Her oncologist had warned her of the risk of immune-related adverse events; MG was one of the rarer ones, occurring in under 1% of patients on her drug. When her eyelid drooping and swallowing difficulty began at week 8 of treatment, the oncology team stopped the immunotherapy and started her on corticosteroids. Her MG resolved over six weeks. Her melanoma remained in remission. She had developed, treated, and recovered from an autoimmune disease in the space of two months as a side effect of cancer treatment. The experience changed how she understood both diseases.