Type 1 Diabetes: The Immune Destruction of Insulin-Making Cells
Type 1 diabetes is not a failure of the pancreas — it is an immune attack on the pancreas. Autoreactive T-cells destroy the beta cells of the islets of Langerhans, eliminating the body's only source of insulin and making exogenous insulin necessary for survival.
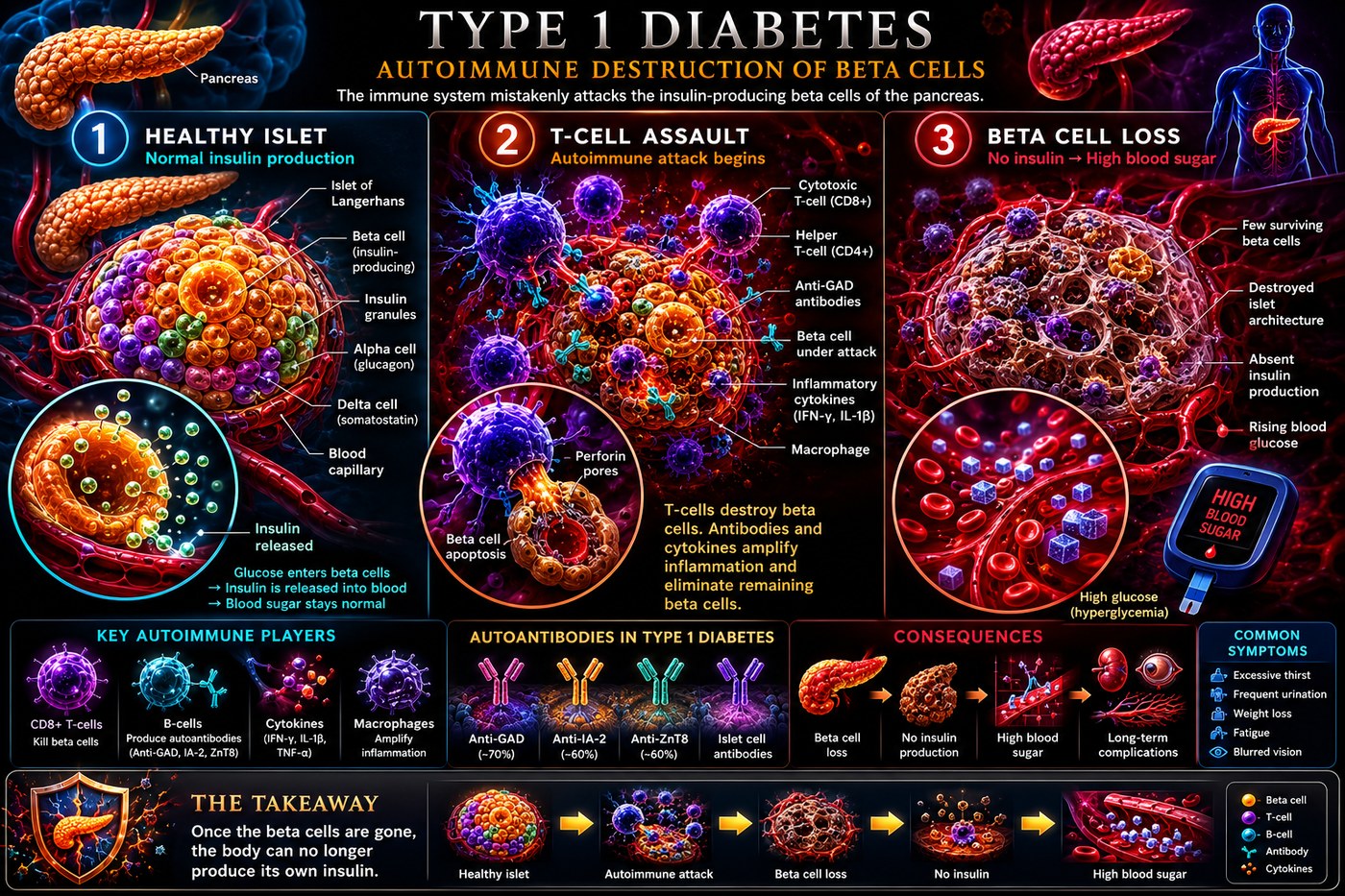
What is happening in the body
The pancreas contains clusters of hormone-producing cells called islets of Langerhans. Within each islet, beta cells are responsible for synthesising and secreting insulin in response to rising blood glucose. In type 1 diabetes, these beta cells are specifically targeted and destroyed by autoreactive CD8+ cytotoxic T-cells in a process called insulitis — immune cell infiltration of the islet.
The autoreactive T-cells recognise beta cell antigens — most notably insulin itself, as well as glutamic acid decarboxylase (GAD65) and zinc transporter 8 (ZnT8) — as foreign. This misdirected recognition is established years before clinical diagnosis. In the pre-diabetic phase, beta cell mass is progressively depleted. When approximately 80–90% of beta cells have been destroyed, insulin secretion falls below the threshold needed to maintain glucose homeostasis and clinical T1D presents — usually abruptly, often as diabetic ketoacidosis in children.
The symptoms this produces
- Polyuria and polydipsia (frequent urination, extreme thirst)
- Rapid, unexplained weight loss
- Fatigue and weakness
- Diabetic ketoacidosis at onset in many cases: nausea, vomiting, deep laboured breathing
- Blurred vision from osmotic changes in the lens
- Long-term: retinopathy, nephropathy, neuropathy, cardiovascular disease
How this fits the autoimmune pattern
Molecular mimicry between bovine serum albumin (BSA) in cow's milk and the beta cell surface protein ICA69 was among the first food-autoimmune connections studied in T1D. Children who were breast-fed longer and introduced to cow's milk later have consistently lower T1D incidence. Wheat gliadin has been shown to increase zonulin and intestinal permeability in people with and without coeliac disease — and T1D patients have two to three times the rate of coeliac disease of the general population, sharing the same gut-driven immune priming mechanism.
What the clinical data shows
Paleomedicina's case series includes children with new-onset T1D whose C-peptide — the marker of residual beta cell function — was preserved and in some cases increased on the PKD, suggesting that when the autoimmune attack is halted early, beta cell regeneration may occur. In longer-standing T1D, the protocol typically results in dramatically reduced insulin requirements due to the near-zero dietary carbohydrate load, with no further autoimmune progression. The PKD's elimination of dairy, wheat, and all permeability-promoting foods removes the antigens driving the molecular mimicry that sustains the autoimmune attack.
A life with this condition — Stories
Liam, 14. His parents brought him to the emergency department after three weeks of constant thirst and unexplained weight loss. His breath smelled sweet. His blood glucose was 34 mmol/L and he was in diabetic ketoacidosis. The diagnosis took six minutes. He was told he would need insulin for the rest of his life, but no one mentioned the years of silent beta cell destruction that had preceded that night — the T-cells entering his islets one by one, the progressive depletion of insulin-producing mass down to the 10% threshold at which the body can no longer maintain glucose control. The crisis was the last chapter, not the first.
Naomi, 31. She was initially diagnosed with type 2 diabetes at 28, given metformin, and told to lose weight. She lost weight — twelve kilograms in six months — and her glucose control deteriorated anyway. Her GP noted that her BMI had always been in the healthy range and referred her to an endocrinologist who tested her GAD65 antibodies. They were strongly positive. She had LADA — latent autoimmune diabetes in adults — a slower-onset form of type 1 where the beta cell destruction unfolds over years rather than months. She had been given advice for a metabolic disease when she actually had an autoimmune one.
Ben, 5. His mother noticed the wet nappies first — heavier than they had ever been, even as a newborn. Then she noticed he was thirsty at night in a way that seemed wrong. She looked up the symptoms on a Saturday afternoon and drove him to the emergency department without waiting for Monday. His glucose was 28 mmol/L; he was starting to slip toward ketoacidosis. The paediatric endocrinologist told her she had probably caught it early enough to avoid the worst of the presentation. Ben was started on insulin that evening. He has worn a continuous glucose monitor every day since. He is now eleven, and the monitor is simply part of his body as far as he is concerned.
Transcript witness — Dr. Anthony Chaffee podcast. A trainer who coached an Olympic T1D athlete: "In my mid-40s I was lucky to train an athlete who had type 1 diabetes. She knew T1D better than anyone I had ever been trained about. She did not follow the guidelines. She did what she thought was best for her, which was keeping carbohydrate essentially at zero. We got her to the Olympics. Her glucose control was the best I had seen in any athlete, diabetic or not. It was only afterward that I started to understand that she had not been ignoring the guidelines out of stubbornness — she had discovered something those guidelines had not caught up with yet."
Isobel, 22. She was the third person in her family with T1D — her mother, her brother, and now her. Her endocrinologist told her that the genetic predisposition meant her immune priming had probably begun in childhood; the only question had been which environmental trigger would tip her over the threshold. She had always been told by relatives that T1D was "just genetics." She was beginning to understand that genetics loaded the gun and something else pulled the trigger, and that the identity of that something else mattered for every other decision she would now make about her health.
Marcus, 38. He had managed his T1D for 24 years when he switched from a multiple daily injection regimen to a closed-loop system — an algorithm linking a continuous glucose monitor to an insulin pump that adjusted delivery automatically. The first morning he woke to a glucose of 5.2 after an overnight run with no intervention on his part, he sat in bed for a long time. He had spent 24 years waking up and immediately calculating. He understood for the first time what people without diabetes experienced as a baseline. He had not known, before that moment, how much cognitive load diabetes had taken from him every single day.
Sofia, 7 — her mother Elena, 35, speaking. "Sofia went into DKA three days before her seventh birthday. She had been sick for weeks and I had taken her to the GP twice. Both times I was told it was a virus. On the third visit I drove straight to the emergency department. Her glucose was 41. We were told she had type 1 diabetes and that she would need insulin for the rest of her life. We were told to go home and wait for a diabetes nurse appointment. We sat in the car park for two hours. She is now nine, she manages her pump herself, she checks her levels at school, and she has never missed a birthday cake. But I have not stopped thinking about those three weeks."