Sjögren's Syndrome: The Slow Drying Out of Glands
Sjögren's syndrome targets the exocrine glands — particularly the salivary and lacrimal glands — with lymphocytic infiltration that destroys the cells responsible for producing saliva and tears. The resulting dryness is progressive, and the systemic inflammation extends beyond the glands.
What is happening in the body
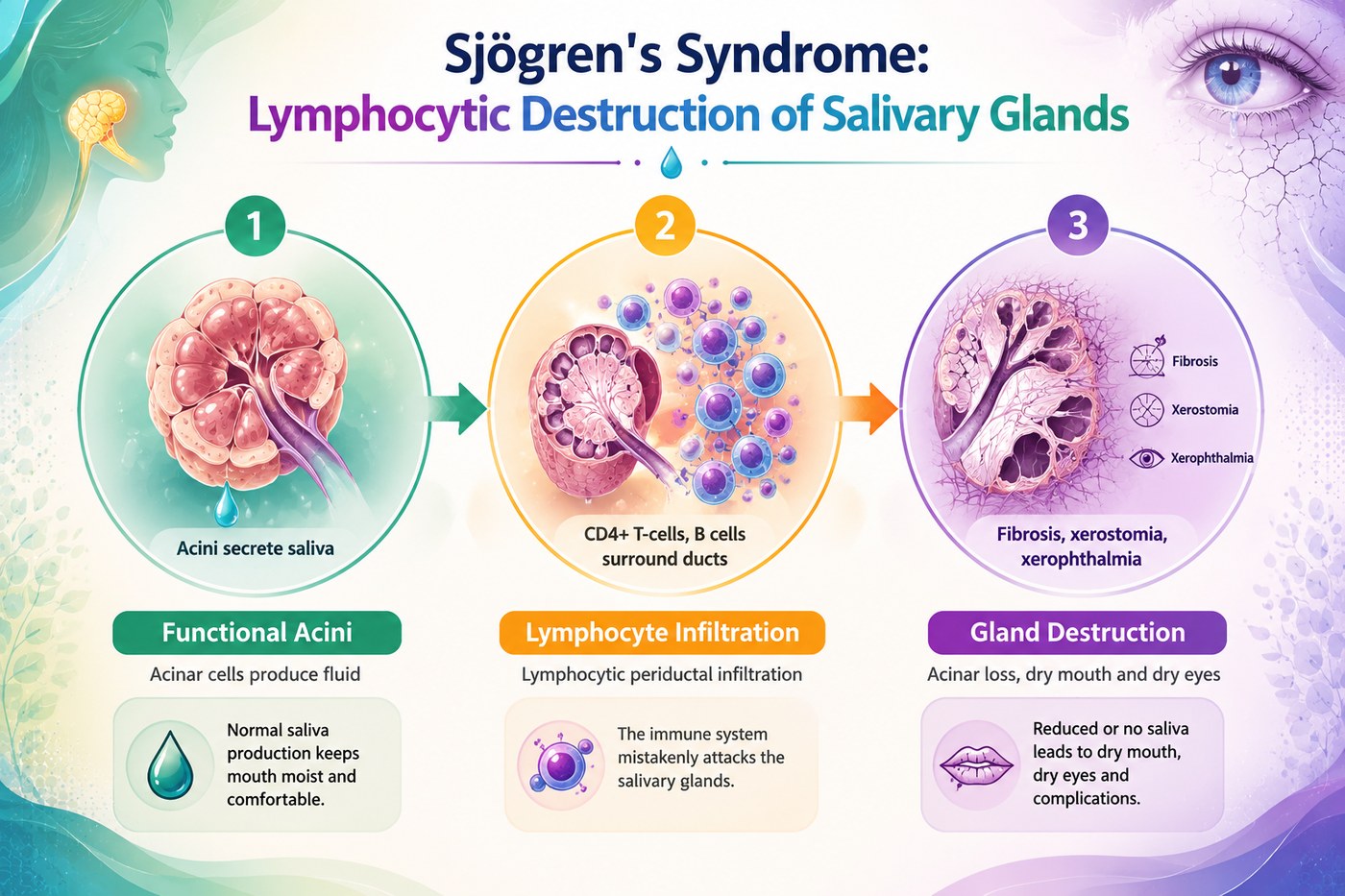
Sjögren's syndrome is classified as an exocrinopathy — a disease of exocrine glands. The salivary glands (parotid, submandibular, sublingual) and lacrimal glands are the primary targets, but any exocrine gland can be involved, including the pancreatic exocrine glands, bronchial mucous glands, and vaginal glands. The glands fill with periductal lymphocytic infiltrates — characteristic foci of 50 or more lymphocytes surrounding each duct — that progressively replace secretory acinar tissue with fibrosis.
The antibodies that define primary Sjögren's — anti-Ro/SSA and anti-La/SSB — target RNA-binding proteins that are exposed on the surface of apoptotic cells. Their pathogenic significance extends beyond the glands: anti-Ro antibodies cross the placenta and can cause congenital heart block in the fetus of a pregnant woman with Sjögren's. Systemically, Sjögren's produces fatigue and arthralgia, and carries a 10–44-fold increased risk of non-Hodgkin lymphoma arising from the chronically activated B cells within the infiltrated glands.
The symptoms this produces
- Xerostomia — dry mouth, difficulty swallowing, dental decay from reduced saliva
- Keratoconjunctivitis sicca — dry, gritty, painful eyes
- Parotid gland enlargement
- Fatigue, often severe
- Arthralgia and myalgia
- Vaginal dryness
- Peripheral neuropathy and autonomic dysfunction in some patients
How this fits the autoimmune pattern
Sjögren's shares the anti-Ro/SSA autoantibody signature with lupus, and the two conditions frequently co-occur. The periductal lymphocytic infiltration suggests a pattern of antigen presentation at ductal epithelial surfaces, primed — as in other autoimmune conditions — by the systemic immune activation that follows intestinal permeability. HTLV-1 and EBV infections are known triggers for Sjögren's through molecular mimicry with salivary gland proteins, demonstrating that the same mechanism operates whether the priming antigen comes from gut or from a pathogen.
What the clinical data shows
Sjögren's syndrome is less frequently reported in the PKD case series than conditions like RA or Crohn's, but patients with secondary Sjögren's (occurring alongside another autoimmune condition) have shown improvement in sicca symptoms when the primary condition responds to PKD. The rationale is reduction in systemic immune activation — the reduction in anti-Ro and anti-La titres parallels the reduction seen in anti-dsDNA in lupus patients, suggesting the same upstream permeability-driven priming mechanism is being addressed.
A life with this condition — Stories
Patricia, 52. She started keeping a water bottle on her desk, then one at her bedside, then one in her car. Her mouth was structurally dry — saliva barely coating the surface, food sticking to the roof of her mouth. Her dentist was alarmed by three new cavities in one year. The lip biopsy her rheumatologist ordered found 47 lymphocytes surrounding each salivary gland duct — immune cells patiently replacing her secretory tissue with scar. She would not produce more saliva than she currently had. She had attributed the dryness to age and air conditioning, not to an immune system quietly dismantling her glands year by year.
Helen, 44. Her Sjögren's presented as fatigue so profound she had reduced her working hours, and a burning, electric pain in her feet she had been told was idiopathic small-fibre neuropathy. The dry mouth and dry eyes she had — she mentioned them almost as an afterthought to her rheumatologist. They were not afterthoughts; they were the diagnostic key. Her anti-Ro/SSA antibodies came back positive; the nerve damage was Sjögren's neuropathy, one of its most debilitating systemic features. For two years she had been treated for symptoms without a named disease. The name, when it arrived, was a relief even though it changed nothing about what had already been damaged.
Anna, 47. She had been managing primary Sjögren's for six years when a neck lump appeared that her rheumatologist could not reassure her about. The lymphadenopathy in Sjögren's patients carries a real and elevated lymphoma risk — the chronically activated B cells within infiltrated glands can undergo malignant transformation. The excision biopsy showed reactive lymphoid hyperplasia, not lymphoma. She was told she had been lucky, and that she would need surveillance indefinitely. Sjögren's had moved from a disease about dryness, which she had learned to manage, to a disease about cancer risk, which she had not anticipated at diagnosis.
Moira, 58. She had been managing Sjögren's for twelve years when she started to lose teeth — not from decay but from the root surfaces fracturing without warning, the result of a decade of xerostomia that had stripped away the protective salivary environment teeth require. Artificial saliva, sugar-free gum, fluoride varnish, scrupulous oral hygiene: she had done everything her dentist recommended. The disease had done more damage faster. She had three implants, bridgework, and a dentist she saw every three months who had become, inadvertently, her most consistent monitor of disease activity.
Yolanda, 46. Her anti-Ro/SSA antibodies had been present on two ANA panels in her thirties, reported by two different GPs as "weakly positive, unlikely to be significant." No one had investigated further. She was 46 when her rheumatologist — reviewing all her blood results at her first appointment — saw the two old positives alongside her current dry eyes and dry mouth and lip biopsy showing 62 lymphocytes per duct. The anti-Ro had been significant for twelve years. The diagnosis had been present in her blood all that time, waiting for someone to read it.
Cyrus, 39. He had primary Sjögren's and peripheral neuropathy that his neurologist initially attributed to idiopathic small-fibre neuropathy. The burning pain in his feet was constant from midday onward and woke him at night. He was treated with pregabalin and duloxetine. It was only when he was referred to a specialist Sjögren's clinic — for unrelated monitoring — that the neurologist there noted that small-fibre neuropathy in Sjögren's is driven by anti-Ro antibody deposition in the dorsal root ganglia. His neuropathy was not idiopathic. It was directly caused by his autoimmune condition. The appropriate treatment targeted the underlying disease, not just the pain signal.
Transcript witness — Dr. Anthony Chaffee podcast. On the shared upstream mechanism across autoimmune conditions: "The same intestinal permeability that drives lupus, RA, and MS is the upstream driver in Sjögren's. The anti-Ro and anti-La antibodies target RNA-binding proteins that become exposed at the surface of apoptotic cells — exactly the kind of cellular debris that floods the systemic circulation when the gut barrier fails. Patients with Sjögren's who address intestinal permeability report improvements in systemic symptoms before the gland-specific symptoms improve — which tells you something about the sequence of events that produces the disease in the first place."