Lupus: When Antibodies Attack Your Own DNA
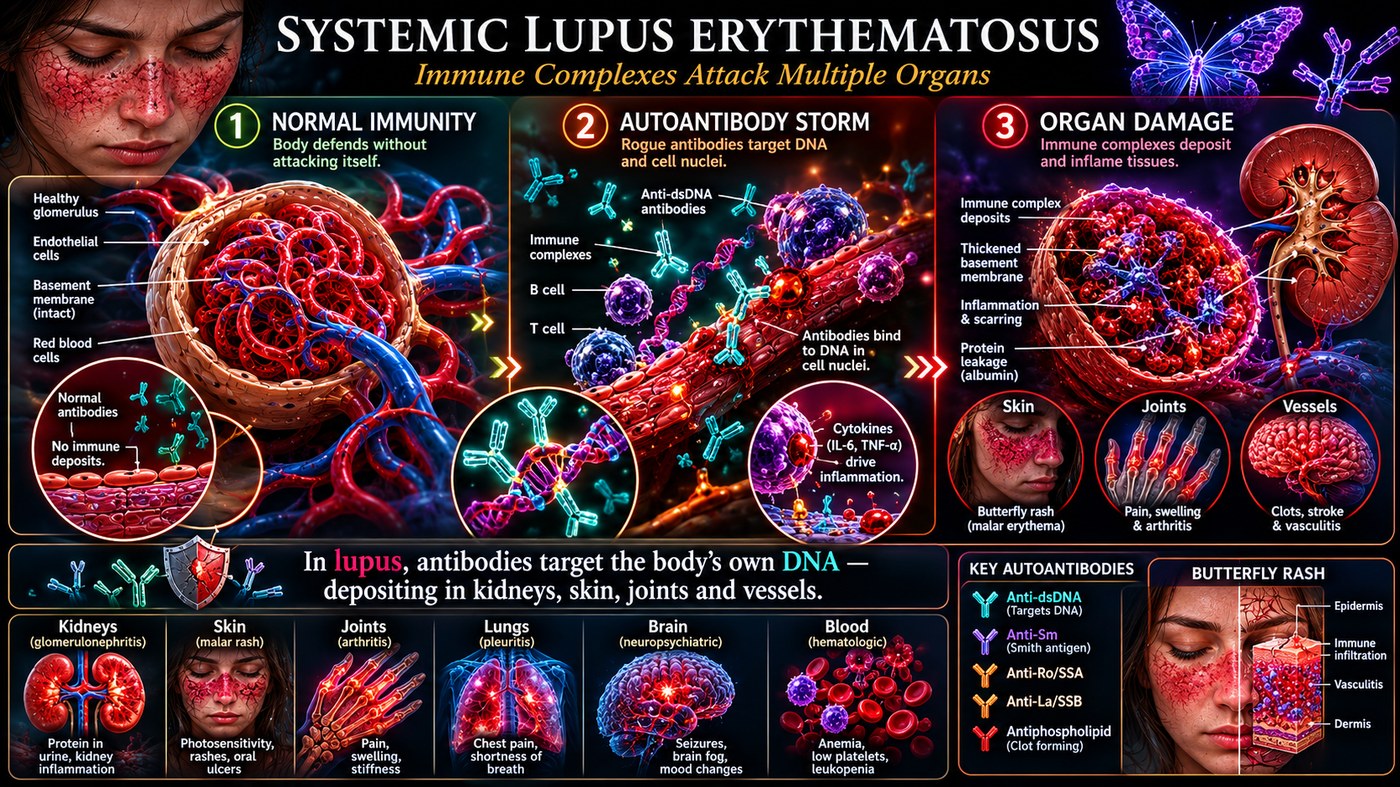
In lupus, the immune system produces antibodies against the body's own DNA. Those antibodies form immune complexes that lodge in the kidneys, skin, and joints — triggering inflammation in organs throughout the body.
What is happening in the body
Systemic lupus erythematosus begins when the immune system fails to clear dying cells efficiently. Fragments of DNA and nuclear proteins from apoptotic cells enter the circulation, and B cells — primed by a loss of tolerance — begin producing antibodies directed at those fragments. The most specific are anti-double-stranded DNA antibodies (anti-dsDNA), which serve as the key diagnostic marker of the disease.
The antibodies do not attack tissue directly. Instead, they bind their targets and form circulating immune complexes — antigen-antibody clusters that are too large for the kidney to filter cleanly. Those complexes lodge in the basement membranes of the kidney's glomeruli, in the capillaries of the skin, in joint linings, and in small blood vessels throughout the body. Once lodged, they activate complement and draw neutrophils, which release tissue-damaging enzymes.
The kidney injury — lupus nephritis — is the most dangerous complication, progressing to kidney failure in a significant minority of patients if untreated. The butterfly-shaped facial rash, joint pain, and fatigue are the more visible but less life-threatening faces of the same underlying immune complex storm.
The symptoms this produces
- Butterfly-shaped malar rash across the cheeks and nose
- Joint pain and swelling (arthralgia, non-erosive arthritis)
- Extreme fatigue and brain fog
- Photosensitivity — rash or flare triggered by sun exposure
- Kidney inflammation (proteinuria, haematuria in nephritis)
- Serositis — inflammation of the lining around the heart and lungs
- Thrombocytopenia, haemolytic anaemia (blood count abnormalities)
How this fits the autoimmune pattern
Lupus illustrates the downstream consequences of impaired self-tolerance. The initial trigger is the failure to clear apoptotic cellular debris — a failure that can be amplified by the same intestinal permeability and systemic immune activation described in the leaky gut model. When food-derived peptides with structural similarities to nuclear proteins reach the systemic immune system repeatedly, they may serve as the initial primer that breaks tolerance to self-antigens.
Patients with lupus have consistently elevated markers of intestinal permeability compared to healthy controls, and dysbiosis — particularly overgrowth of certain Proteobacteria — is a reproducible finding. The carnivore and PKD protocol removes the dietary sources of gut barrier disruption and eliminates cross-reactive plant lectins, addressing the upstream driver rather than suppressing the downstream antibody response.
What the clinical data shows
Case series from Paleomedicina Hungary document lupus patients achieving sustained clinical remission on the Paleolithic Ketogenic Diet. In one published case, a 23-year-old woman with biopsy-confirmed lupus nephritis — on hydroxychloroquine and mycophenolate — achieved normalization of all renal parameters and negative anti-dsDNA titers within six months of adopting PKD, subsequently tapering all medication. Complement C3 and C4, chronically suppressed, normalized. The mechanism proposed is elimination of the gut permeability that continuously feeds antigenic material into the systemic circulation.
A life with this condition — Stories
Sarah, 23. Her face swelled overnight — both cheeks flushed in a butterfly pattern that her GP photographed and sent to a dermatologist the same afternoon. Before that she had been dizzy for two weeks and had lost four kilograms without trying. The blood tests came back showing her kidneys were inflamed; she was started on hydroxychloroquine and told to avoid sunlight. For the next three years, every spring flare arrived on schedule, triggered by an afternoon in a garden or a weekend at the coast. What no one explained clearly was that her immune system had decided her own DNA was an invader — and that the butterfly rash was the least dangerous part of what was happening.
Marcus, 40. He had been told for three years that his joint pain was from old sporting injuries. He was a former semi-professional footballer and the diagnosis felt plausible. It was only after he developed pleuritis — a stabbing chest pain that worsened with every breath — that his GP ordered the full autoimmune panel. His anti-dsDNA came back at 1:640. He had lupus. Looking back, the fatigue he had attributed to age, the mouth ulcers he had dismissed as stress, and the occasional facial flushing he had blamed on alcohol were all part of the same disease. He had been living with it for years without a name for it.
Aiko, 35. Her lupus presented not with a rash but with a platelet count of 28,000 — low enough to cause spontaneous bruising across her forearms that her haematologist initially investigated as a blood cancer. The bone marrow biopsy came back normal. It was the haematologist who ordered the ANA panel on a hunch, and it came back at 1:1280 with anti-dsDNA positive. Aiko had never had a rash. She had haemolytic anaemia and thrombocytopenia — her immune system attacking her blood cells with the same antibodies it directed at her kidneys. She had assumed the bruises were from the iron deficiency she already knew about. They were not.
Diana, 28. Her lupus came for her joints first — both wrists, both ankles. She was told it was probably viral arthritis and given anti-inflammatories. Six weeks later she developed pleuritis and her GP finally ordered an ANA panel. It came back at 1:2560. She had never had the butterfly rash. She had been told she was "too young" for a serious connective tissue disease. Her rheumatologist told her that was a common reason lupus goes undetected in young women: the textbook rash is only present in about half of cases, and without it, the diagnosis is easily missed.
Jerome, 45. He was referred to rheumatology after his fourth episode of unexplained pericarditis — inflammation of the sac around the heart. Each episode had been treated as idiopathic. Nobody had connected them. The autoimmune workup found anti-Smith antibodies, highly specific for lupus. He had been having pericarditis attacks for seven years. The disease had been visible every time, in the one organ no one had thought to connect to an immune condition.
Camille, 19. She was in her first year of university when fatigue became so total she could not get from her dormitory bed to lectures. She slept twelve hours and woke unrefreshed. Her joints ached. Her hair came out in clumps in the shower. She was investigated for anaemia, thyroid disease, and depression before haematology found haemolytic anaemia. The ANA was positive; the anti-dsDNA confirmed lupus. The fatigue pathologised as anxiety was her immune system running at full activation against her own red blood cells and nuclear proteins simultaneously.
Transcript witness — Dr. Anthony Chaffee podcast. A clinician who works with fibromyalgia and lupus patients: "The pain is astronomical, if I am being real. I have had a lot of success in helping people do much better with lupus on a meat-based approach. What I notice is that the pain starts to shift within the first few weeks, and then over months, the antibody picture begins to change. I have seen anti-dsDNA titres fall. I have seen complement come back up. I was taught this was not possible."
Renata, 33. Her first rheumatologist told her she had fibromyalgia and offered antidepressants. Her second rheumatologist, three years later, ordered an anti-Smith antibody panel after noticing her ANA titre had been sitting at 1:160 in records from multiple previous visits that no one had followed up. The anti-Smith came back positive. She had been managing a mis-labelled disease for three years, adjusting her life around pain that everyone around her was effectively telling her was not real.
Yuki, 41. Her lupus went into remission on her own — rare, but documented — and she came off hydroxychloroquine after five years. Two years later it returned, triggered by the combination of a viral illness and a period of significant psychological stress. Her rheumatologist restarted medication and noted that while the trigger was the infection, the vulnerability was still there. Remission in lupus is conditional, not cured. She had learned that during the years of remission she had begun to treat herself as healthy in a way that was not entirely accurate.