Hashimoto's Thyroiditis: When the Immune System Silences the Thyroid
Hashimoto's thyroiditis is the most common cause of hypothyroidism in the developed world. Lymphocytes infiltrate the thyroid gland, destroying follicles and replacing functional tissue with fibrosis — progressively silencing the gland's ability to produce thyroid hormone.
What is happening in the body
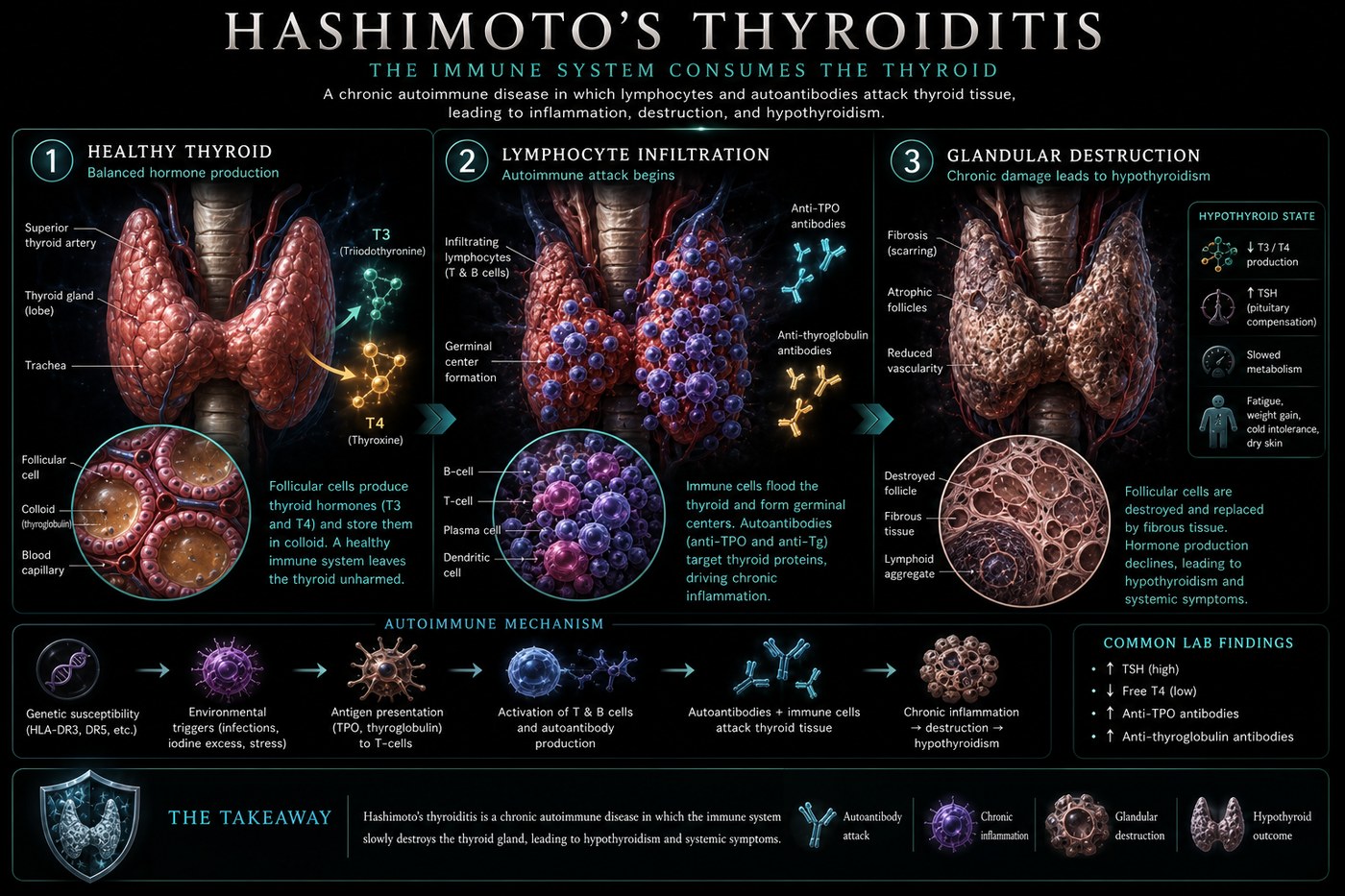
The thyroid gland is organised into spherical follicles, each lined with thyrocytes and filled with colloid — a gel containing thyroglobulin, the precursor from which T3 and T4 are cleaved. In Hashimoto's, this architecture is progressively dismantled by lymphocytic infiltration. Both CD4+ helper T-cells and CD8+ cytotoxic T-cells accumulate within the gland, forming germinal centres — the organised lymphoid structures normally found in lymph nodes — within the thyroid tissue itself.
B cells within those germinal centres produce the antibodies that are the clinical hallmarks of the disease: anti-thyroid peroxidase (anti-TPO) and anti-thyroglobulin (anti-TG). Thyroid peroxidase is the enzyme that iodinates thyroglobulin, the first step in thyroid hormone synthesis; antibodies against it impair hormone production. The cellular immune attack simultaneously destroys follicular cells. Over years, functional follicular tissue is replaced by fibrosis, the gland shrinks, and the hypothalamic-pituitary axis compensates by driving TSH higher — producing the elevated TSH that typically first signals the disease.
The symptoms this produces
- Fatigue disproportionate to rest (often the first symptom)
- Weight gain despite unchanged diet
- Cold intolerance
- Slow pulse, constipation
- Brain fog and depression
- Dry skin and hair loss
- Goitre (enlarged thyroid) in some patients; atrophic gland in others
How this fits the autoimmune pattern
Hashimoto's shares the autoimmune terrain of increased intestinal permeability and molecular mimicry. Gliadin and thyroid antigens share structural peptide sequences, and the correlation between coeliac disease and Hashimoto's — approximately three times the expected coeliac rate among Hashimoto's patients — points to shared gut-mediated immune activation. A published randomised trial showed that a strict gluten-free diet significantly reduced anti-TPO and anti-TG titres in Hashimoto's patients without coeliac disease, confirming the wheat-thyroid immune axis.
What the clinical data shows
Paleomedicina case series document Hashimoto's patients tapering and eventually discontinuing levothyroxine after antibody normalisation on the PKD. In one published case, a woman with 16 years of Hashimoto's thyroiditis and dependence on thyroid supplementation achieved normal TSH, T3, and T4 levels without medication after eight months on PKD, with anti-TPO declining from several hundred to within normal range. The mechanism is removal of all dietary triggers for gut permeability and thyroid-cross-reactive immune activation.
A life with this condition — Stories
Claire, 34. She had been told she was depressed for two years before her new GP ordered a thyroid panel. She was not depressed. She was cold when no one else was cold, exhausted after eight hours of sleep, gaining weight on a diet that should have maintained her. Her brain felt like it was running through mud. Her TSH came back at 18; her anti-TPO antibodies were 640 IU/mL. The thyroid ultrasound showed a gland with the moth-eaten texture of established Hashimoto's. She had not been depressed. She had had a slowly failing organ, and had been sent to psychiatrists instead of endocrinologists.
Sandra, 38. Her Hashimoto's was triggered, her endocrinologist believed, by the immune rebound after pregnancy. She had been fine throughout her pregnancy — thyroid autoimmune conditions often improve during gestation as immune tolerance increases. Six weeks postpartum, the suppression lifted, the immune system surged, and her anti-TPO antibodies quadrupled. She had attributed the exhaustion, the hair falling out in the shower, and the inability to feel warm to having a newborn. It was only when her baby was six months old and the symptoms had not improved that her midwife ordered the test.
Michael, 62. His Hashimoto's had been managed on levothyroxine for eleven years when he developed a goitre large enough to cause mild difficulty swallowing. His endocrinologist explained that some Hashimoto's patients develop enlargement rather than atrophy — the immune infiltration provoking a paradoxical growth response. His TSH was controlled on medication, his antibodies remained elevated, and his thyroid was simultaneously being attacked and attempting to compensate by growing. He found the contradiction difficult to explain to family members who assumed that being "on medication for it" meant the disease was resolved.
Transcript witness — Dr. Anthony Chaffee podcast. A practitioner with over 100 Hashimoto's patients: "I see so many people who are hypothyroid and I have over 100 patients with Hashimoto's. Not even getting into the whole estrogen side of things — there are so many reasons why a carnivore diet improves thyroid function. Hashimoto's is the most common autoimmune condition I treat, and it is one of the most responsive to dietary intervention. I have seen anti-TPO titres fall from the hundreds to within normal range. I have seen patients come off levothyroxine. I was not taught that was possible. I am seeing it anyway."
Nadia, 29. Her Hashimoto's was found incidentally when her GP ordered a thyroid panel as part of a general fatigue workup. Her TSH was mildly elevated at 6.2; her anti-TPO was 380. She had no symptoms she had thought to mention — the fatigue was "just life," the cold was "just how she was," the dry skin was "just winter." Her GP told her she might not need medication yet, but to monitor. She started monitoring and discovered that with each check over two years her TSH climbed — 7.4, then 9.1 — and her symptoms she had normalised became ones she could not. She started levothyroxine on the third check and felt, for the first time in years, like herself.
Olga, 44. She removed gluten from her diet after reading a randomised trial showing anti-TPO titres falling significantly in Hashimoto's patients on a gluten-free diet — without coeliac disease being present. Her gastroenterologist had told her the trial was too small. Her endocrinologist had said the evidence was insufficient to recommend. She removed it anyway. Her anti-TPO dropped from 520 to 180 over eight months. She brought the results to her endocrinologist, who said they were "encouraging." She asked whether she should put gluten back to confirm causality. He said that was her decision. She did not put it back.
Freya, 55. She had been on levothyroxine for sixteen years and felt adequately managed — until she discovered that "adequately managed" had a different meaning to her endocrinologist than to her. Her TSH was in range, which her endocrinologist considered the goal. She had persistent fatigue, persistent brain fog, and persistent weight gain that did not resolve on the medication. A functional medicine doctor ordered T3 alongside TSH and found her free T3 was in the low normal range despite normal TSH. She added liothyronine. The brain fog lifted within three weeks. She had been in range. She had not been well.