Graves' Disease: Antibodies That Force the Thyroid Into Overdrive
Graves' disease is the mirror image of Hashimoto's: instead of destroying the thyroid, the immune system produces antibodies that mimic TSH and lock the gland into permanent stimulation. The result is uncontrolled hyperthyroidism — a runaway metabolic acceleration.
What is happening in the body
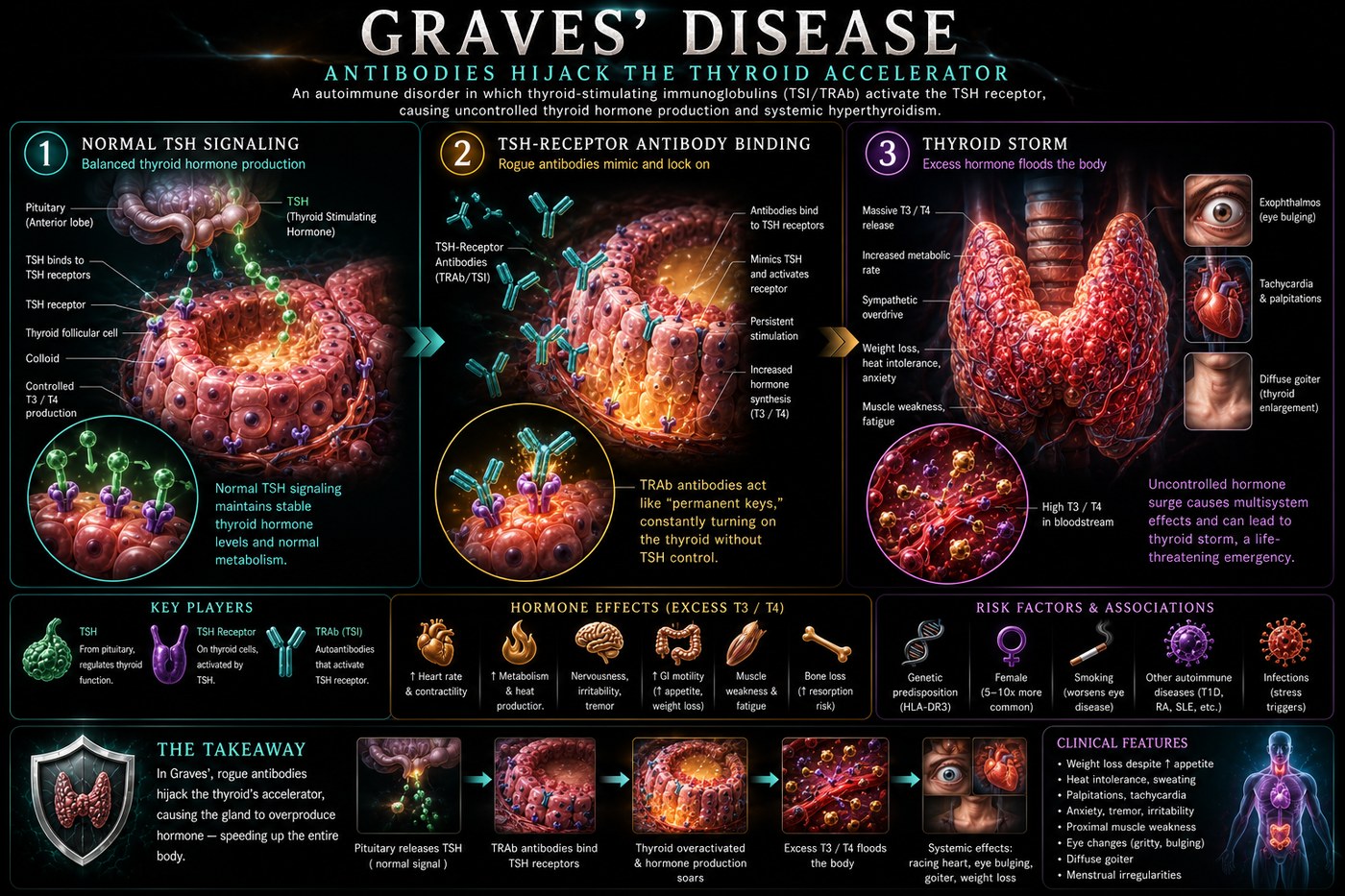
The thyroid gland is regulated by a feedback loop: the pituitary secretes TSH, which binds to TSH receptors on thyrocytes, stimulates hormone synthesis, then releases. Circulating T3 and T4 feed back to suppress TSH when levels are adequate. In Graves' disease, the immune system produces thyroid-stimulating immunoglobulins (TSI) — antibodies that bind the TSH receptor in the same site as TSH but cannot be cleared by the normal feedback mechanism.
Unlike TSH, which binds and releases as levels fluctuate, TSI stays bound. It constitutively activates the receptor's downstream signalling cascade — adenylyl cyclase, cAMP, PKA — driving thyroid hormone synthesis continuously and without restraint. The pituitary responds by suppressing TSH to almost undetectable levels, but the antibody-driven stimulation ignores that suppression. The gland enlarges (diffuse goitre), vascularity increases, and T3 and T4 rise to levels that accelerate every metabolic process in the body.
Graves' ophthalmopathy — the eye protrusion characteristic of the disease — is caused by TSI cross-reacting with TSH receptors in orbital fibroblasts, causing glycosaminoglycan accumulation and inflammatory expansion of the retroorbital tissue.
The symptoms this produces
- Palpitations and rapid heart rate (tachycardia, sometimes atrial fibrillation)
- Heat intolerance and excessive sweating
- Weight loss despite increased appetite
- Tremor in the hands
- Proptosis (exophthalmos) — protruding, staring eyes
- Anxiety, irritability, insomnia
- Diarrhoea and frequent bowel movements
How this fits the autoimmune pattern
Graves' and Hashimoto's share the same underlying terrain of thyroid autoimmunity and can coexist in the same patient or family. The TSI-producing B cells require T cell help — specifically Th2-polarised responses — suggesting the same gut-mediated immune dysregulation that drives other autoimmune conditions. Iodine excess is an established environmental trigger, as is psychological stress, through cortisol-mediated immune modulation. Gut permeability and molecular mimicry between gut-derived antigens and thyroid tissue remain the upstream drivers.
What the clinical data shows
Graves' disease is less extensively studied in the PKD literature than Hashimoto's, but Paleomedicina has documented cases of TSI normalisation and hyperthyroidism remission in patients adopting the PKD. The diet eliminates the dietary triggers of both permeability and Th2 immune skewing while providing the nutrient density (selenium, zinc, iodine through seafood and organ meats) required for normal thyroid function. Several patients have avoided radioiodine ablation or thyroidectomy by achieving immunological remission through dietary intervention.
A life with this condition — Stories
Tom, 45. His wife asked why his eyes looked different. He had noticed his heart racing but attributed it to caffeine; he had dropped six kilograms while eating more than usual, which he had found gratifying. His optometrist noticed the proptosis during a routine check — both eyes slightly prominent, lids retracted — and referred him immediately. TSH was undetectable; TSI antibodies were strongly positive. Antibodies that mimicked TSH but never released from the receptor were driving his thyroid continuously, regardless of how high his hormone levels climbed. He had felt energetic. He had been burning himself from the inside.
Lucy, 32. She had been treated for panic disorder for eight months when her cardiologist finally ordered a thyroid panel. She had presented repeatedly with palpitations, racing heart, and anxiety so severe she had stopped going to social events. The psychiatrist had started her on an SSRI. Her T3 was 9.2 pmol/L — nearly double the upper limit. Her TSI antibodies confirmed Graves'. The "panic attacks" were thyrotoxicosis — her hyperstimulated thyroid flooding her body with hormone that accelerated every cardiac and neurological process she had. The SSRI was stopped. Carbimazole was started. Within three months she felt, for the first time in a year, like herself.
Paul, 59. He had known about his Graves' disease and was stable on low-dose carbimazole when he needed a contrast CT scan for an unrelated matter. Within 72 hours of the iodine contrast injection, he was in the emergency department with a heart rate of 148 and a temperature of 39.2°C. His endocrinologist confirmed thyroid storm — an acute, life-threatening surge of thyroid hormone triggered by the iodine load hitting a gland that was already autonomously overactive. He spent four days in the ICU. It was the first time he understood that his disease, which had felt managed and minor, could still kill him without warning.
Transcript witness — Dr. Anthony Chaffee podcast. On the mechanism of Graves' and dietary intervention: "If the lectins or food-derived antigens are triggering the antibody response that stimulates the TSH receptor, then when you remove those triggers, over time those antibodies will come down. I have seen that with Hashimoto's and Graves'. With Graves', the symptoms — the palpitations, the tremor, the heat intolerance — start to ease before the antibody titres formally normalise. People often feel better and think they have recovered. The titres catch up later. The sequence matters: symptoms first, then antibodies, in that order."
Mei, 27. She was hyperthyroid throughout her pregnancy and her obstetrician and endocrinologist managed her carefully with low-dose propylthiouracil, which crosses the placenta less than carbimazole. Her baby was born at term, healthy, with normal thyroid function. What her endocrinologist told her afterward was that pregnancy often temporarily improves Graves' disease through the immune tolerance mechanisms that protect the fetus from maternal immunity, but that the postpartum period carries a high relapse risk as those mechanisms lift. The remission she had felt during the second trimester was real. It was also temporary. She relapsed at ten weeks postpartum, as her endocrinologist had predicted.
Elijah, 53. He chose radioiodine ablation after two years on antithyroid drugs — his endocrinologist's preferred option for long-term management. He became hypothyroid within six months of the ablation, which was the expected outcome: the radioiodine destroyed enough thyroid tissue to eliminate the hyperthyroidism, and he then needed levothyroxine for the rest of his life. He had traded one thyroid disease for another, which was the intended result, and was managing well. What he had not been fully prepared for was the permanent nature of that trade. He had assumed "getting rid of" the hyperthyroidism meant being done with thyroid problems. It did not.
Adaeze, 31. Her Graves' disease presented first as infertility. She and her husband had been trying to conceive for eighteen months when her reproductive endocrinologist ordered a comprehensive hormonal panel and found suppressed TSH and elevated free T4 alongside elevated TSI. Thyrotoxicosis impairs fertility by disrupting the LH surge and disrupting progesterone production in the luteal phase. Her reproductive endocrinologist referred her to an endocrinologist for thyroid control before further fertility treatment. Within four months of achieving euthyroid status on carbimazole, she conceived naturally. The disease that had been blocking her fertility had been invisible in every workup that had not included the thyroid.