Crohn's Disease: Inflammation That Eats Through the Gut Wall
Crohn's disease is a transmural inflammation — it burns through the full thickness of the intestinal wall. Unlike ulcerative colitis which is limited to the surface, Crohn's can penetrate to neighbouring organs, forming abscesses and fistulas while the immune system mistakes gut bacteria for invaders.
What is happening in the body
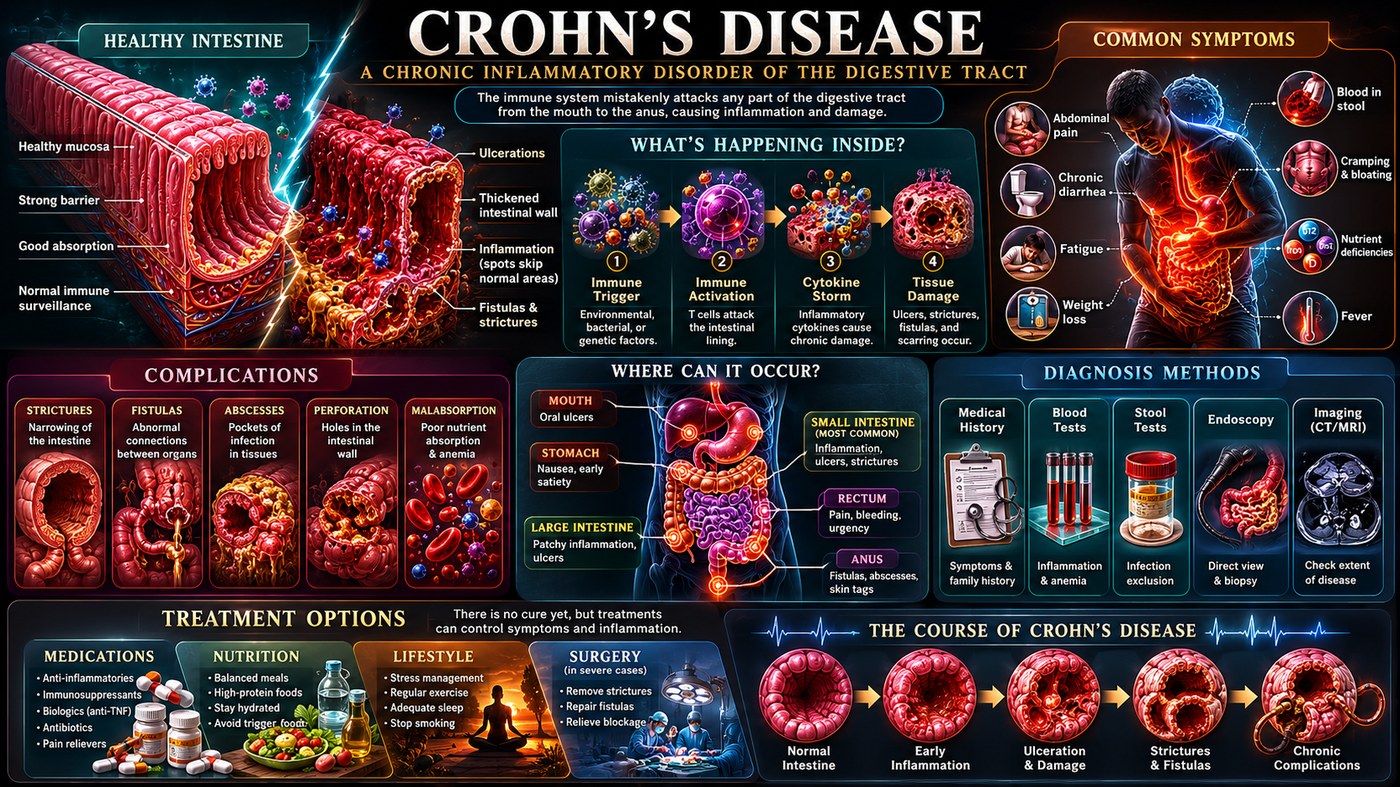
Crohn's disease is defined by its transmural character: the inflammation does not stay on the surface of the intestinal lining but penetrates through every layer of the gut wall — mucosa, submucosa, muscularis propria, and serosa. This distinguishes it sharply from ulcerative colitis, which remains mucosal. The transmural spread is why Crohn's produces fistulas (abnormal tunnels connecting loops of bowel or bowel to bladder, vagina, or skin) and abscesses, while UC does not.
The hallmark histological finding is the granuloma — a structured collection of macrophages and epithelioid cells attempting to wall off what the immune system perceives as an unresolvable foreign body. In Crohn's, that perceived foreign body is intestinal bacteria. The normal gut immune system maintains tolerance to luminal bacteria through a complex balance of regulatory signals. In Crohn's, that tolerance collapses — particularly in genetically susceptible individuals with NOD2 mutations that impair bacterial sensing in Paneth cells — and macrophages mount an unregulated response to normal commensal organisms.
The result is skip lesions — patches of severe inflammation separated by normal tissue — that can occur anywhere from mouth to anus, though the terminal ileum and proximal colon are most commonly affected.
The symptoms this produces
- Cramping abdominal pain, often right lower quadrant
- Chronic diarrhoea, sometimes bloody
- Weight loss and malnutrition from malabsorption
- Perianal fistulas and abscesses
- Fever during flares
- Extra-intestinal manifestations: mouth ulcers, skin lesions (erythema nodosum), eye inflammation, arthritis
- Growth retardation in children
How this fits the autoimmune pattern
Crohn's is the most direct expression of the leaky gut mechanism. The disease begins at the intestinal barrier, and its pathology is entirely driven by abnormal immune responses to luminal contents. Increased intestinal permeability precedes clinical onset and is present in unaffected first-degree relatives of Crohn's patients — suggesting it is a disease driver, not merely a consequence. The foods associated with Western dietary patterns — grains, refined carbohydrates, seed oils — are the primary drivers of that permeability increase.
What the clinical data shows
Paleomedicina's most dramatic published case involves a young man with severe Crohn's disease facing bowel resection surgery who achieved complete endoscopic and histological remission on the PKD within months, avoiding surgery entirely. The protocol's complete elimination of plant-based foods removes all sources of intestinal permeability-promoting lectins and phytates while providing the L-glutamine and butyrate precursors the gut lining requires for repair. Multiple Crohn's patients have been documented reaching drug-free remission with negative CRP and calprotectin on PKD.
A life with this condition — Stories
Daniel, 32. He spent three years diagnosed with IBS before his gastroenterologist said "that's not IBS" within seconds of reaching the terminal ileum during his first colonoscopy. The ulcers were deep craters punched through all layers of the gut wall. He had lost eleven kilograms and attributed it to stress. What he actually had was a fistula forming between two loops of bowel that a CT scan had already detected but a previous doctor had called "non-specific." The mechanism — macrophages forming granulomas around gut bacteria they could no longer tolerate — was abstract against the concrete reality of a perianal abscess drained at two in the morning.
Sophie, 16. Her Crohn's presented as failure to thrive. She was shorter than expected, not gaining weight, missing school because of abdominal pain she had been told was anxiety. Her paediatrician finally referred her to a paediatric gastroenterologist who looked at her growth chart — flat for two years — and ordered a faecal calprotectin test. It came back at 1,840 µg/g, twelve times the normal limit. The colonoscopy showed skip lesions from the terminal ileum into the ascending colon. She had been living with active intestinal inflammation throughout her most critical years of development.
Ahmed, 41. He had been operated on three times in five years — two perianal fistula repairs and one bowel resection — before he found a gastroenterologist who explained that surgery treats the consequences of Crohn's but not the disease itself. Without controlling the underlying immune response, fistulas recur and bowel segments re-inflame. His life had been structured around proximity to bathrooms, around predicting which meals would trigger pain, around estimating how far he could walk from any given point before needing to stop. The disease had not been unmanaged; it had been managed only at the level of its wreckage.
Transcript witness — Dr. Anthony Chaffee podcast. A physician describing randomised controlled trial evidence: "There are studies going back to 1984, 1985, 1987 showing that removing carbohydrates and fibre can put Crohn's disease into remission for up to 51 months without medication. The control group that did not remove carbohydrates and fibre could not even stay in remission. Why is this not taught in gastroenterology training? Why does a person with Crohn's have to find this on their own? These are not fringe findings. They are published, randomised, controlled trials."
Tomas, 27. He had Crohn's that responded initially to azathioprine and then stopped responding. His gastroenterologist moved him to a biologic and he had three good years before developing antibodies to that drug too. This was the pattern his gastroenterologist described as "step therapy" — each medication working for a period, then failing. He asked at each step what he could do with his diet. At each step he was told diet would not make a significant difference. It was only when he looked outside his hospital that he found people who had stopped the step therapy at step one by removing the foods that appeared to drive his inflammation.
Ingrid, 35. Her Crohn's fistula had been repaired surgically and was holding. Her gastroenterologist was pleased with her imaging. What he could not see was that Ingrid had quietly eliminated all grains, legumes, and processed foods from her diet six months earlier after reading about a clinical case series from Hungary. Her CRP — previously elevated at 48 — was now 3. She did not volunteer this information at her appointments for nearly a year, afraid she would be told to stop. When she finally told her gastroenterologist, he reviewed her bloods, reviewed her imaging, and said: "Whatever you are doing, keep doing it."
Kwame, 21. He was diagnosed during his university entrance exams. The timing meant that alongside learning he had a chronic disease, he was making decisions about university courses around proximity to hospitals, the likelihood of surgery, the feasibility of gap years. He eventually chose a university near a specialist IBD unit and deferred his start by a year. His gastroenterologist told him that with good management, Crohn's need not define his career. What the gastroenterologist did not mention was what "good management" had historically meant for people like Kwame — and what it was beginning to mean now.