Celiac Disease: How Gluten Destroys the Intestinal Villi
Celiac disease is the one autoimmune condition with a completely identified dietary trigger: gliadin, the alcohol-soluble fraction of wheat gluten. In genetically susceptible individuals, gliadin initiates an immune cascade that flattens the intestinal villi and impairs absorption of nearly every nutrient.
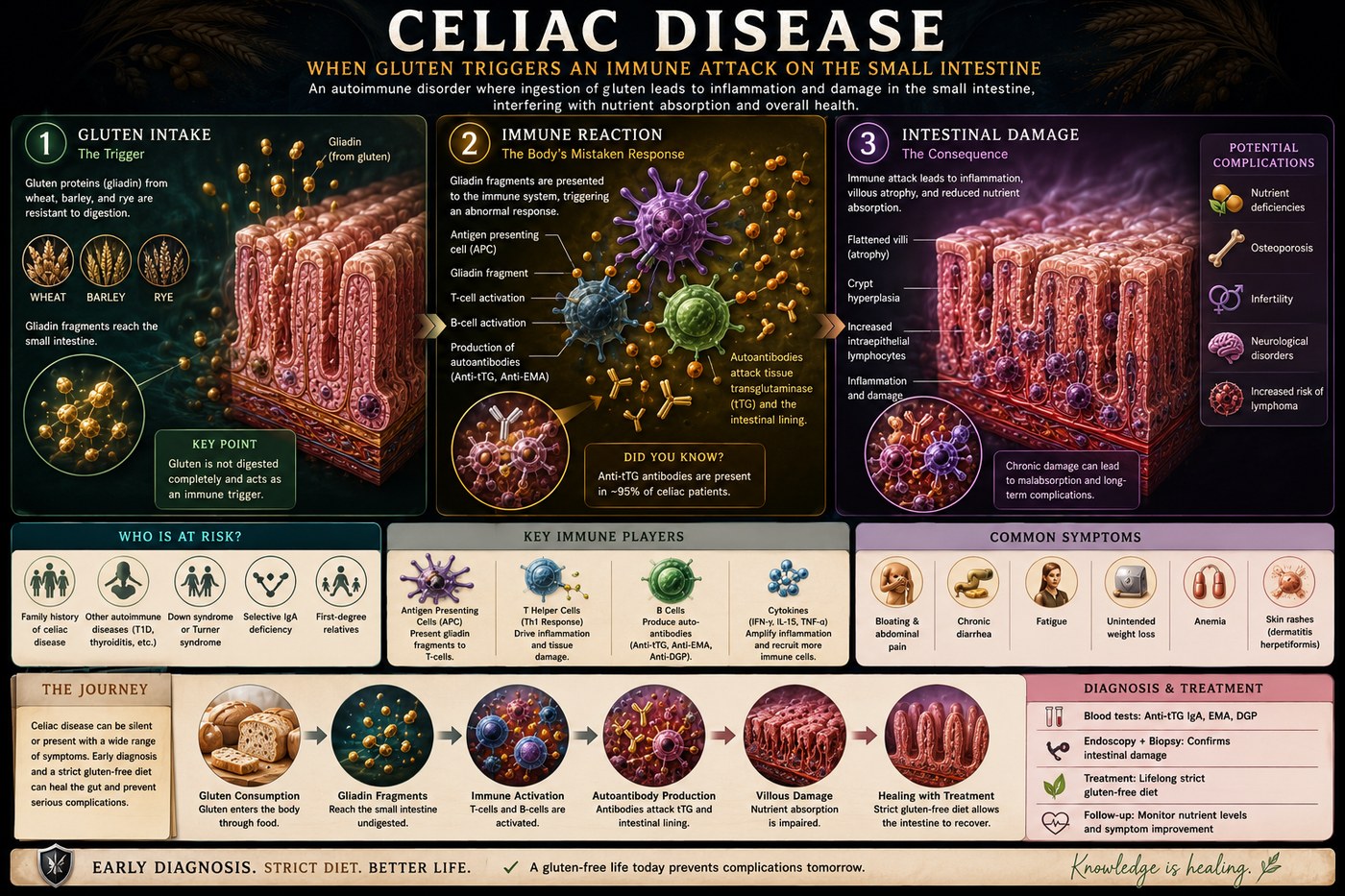
What is happening in the body
In celiac disease, the immune trigger is precisely identified: alpha-gliadin, a protein in wheat (and related prolamins in rye and barley). In genetically susceptible individuals carrying HLA-DQ2 or HLA-DQ8 — present in 98% of celiac patients — gliadin peptides that survive digestion enter the lamina propria through a leaky epithelial barrier. There, the enzyme tissue transglutaminase (tTG) deamidates gliadin peptides, converting glutamine residues to glutamate and increasing their affinity for HLA-DQ2/DQ8 molecules on antigen-presenting cells.
The resulting T-cell activation drives a dual immune response: a Th1-mediated cytotoxic attack on enterocytes and a B-cell antibody response producing the IgA anti-tTG antibodies used for diagnosis. CD8+ intraepithelial lymphocytes kill villous enterocytes, while cytokine release drives crypt hyperplasia — a compensatory but inadequate attempt to replace the destroyed absorptive surface. Over time, the villi flatten (partial to total villous atrophy), drastically reducing the absorptive surface area of the small intestine.
The symptoms this produces
- Chronic diarrhoea and steatorrhea (fatty, malodorous stools)
- Abdominal bloating, pain, and distension
- Weight loss and failure to thrive in children
- Iron-deficiency anaemia unresponsive to supplementation
- Osteoporosis from calcium malabsorption
- Dermatitis herpetiformis — the skin manifestation
- Peripheral neuropathy and ataxia (gluten neuropathy)
How this fits the autoimmune pattern
Celiac disease is the autoimmune condition that most directly validates the leaky gut model because the sequence is fully established: wheat → intestinal permeability increase (via zonulin) → gliadin entry → tTG deamidation → immune activation → villous destruction. Remove wheat entirely and the immune response resolves, the villi regenerate, and the antibodies normalise. Celiac disease demonstrates that the same dietary factors proposed as drivers of other autoimmune conditions can, in the right genetic context, directly cause autoimmune tissue destruction.
What the clinical data shows
Unlike most autoimmune conditions, celiac disease has an established, guideline-recommended dietary treatment: strict lifelong gluten elimination. Mucosal healing confirmed by repeat biopsy occurs in 80–95% of patients who achieve complete dietary compliance. The PKD, which eliminates all grains by design, achieves this as a baseline. In Paleomedicina patients with co-existing celiac and another autoimmune condition, both conditions have been shown to respond simultaneously to the PKD protocol.
A life with this condition — Stories
Noah, 14. He had anaemia from age 11 that no iron supplement could hold. He was tired, short, not thriving in sports. At 14 a new paediatrician tested anti-tTG IgA and called his mother the same day. The biopsy showed total villous atrophy — the intestinal absorptive surface reduced to a fraction of normal. His immune system had been attacking his own intestinal cells every time he ate bread, and he had been eating bread with every meal for as long as he could remember. He stopped eating wheat completely. Within a year he was in the 60th percentile for height and his ferritin stayed normal without supplementation for the first time in his life.
Diana, 41. Her celiac disease presented not with gut symptoms but with ataxia — a progressive unsteadiness when walking that had baffled three neurologists over two years. Her brain MRI was normal; her nerve conduction studies showed a mild peripheral neuropathy. It was a fourth neurologist who knew about gluten ataxia — the neurological form of celiac disease, in which anti-gliadin antibodies damage the cerebellum and peripheral nerves rather than the intestine — who ordered the anti-tTG panel. Her titre was 340 U/mL. She had never had significant diarrhoea. Her gut was her warning sign that no one had read.
Patrick, 54. He was asymptomatic. He only tested because his sister had been diagnosed with celiac disease the month before, and his gastroenterologist recommended first-degree relatives be screened. His anti-tTG came back positive; his biopsy showed partial villous atrophy. He had no gut symptoms, no fatigue he had attributed to anything specific, no anaemia. What he did have, his GP noted on reviewing his records, was a DEXA scan from three years earlier showing osteoporosis — unexplained at the time — in a man with no obvious calcium deficiency. The malabsorption had been silently removing calcium from his bones for years while he felt entirely well.
Transcript witness — Dr. Anthony Chaffee podcast. On the diagnostic precision of celiac disease: "Celiac is called an autoimmune disease, but it is actually the clearest demonstration that so-called autoimmune diseases are not the immune system attacking itself at random — they are the immune system responding to a specific antigen that should not be present. Remove the antigen, the immune response stops. The tissue heals. The antibodies normalise. This is not mysterious. It is antigen removal. The only reason we do not apply this logic to all autoimmune conditions is that we have not identified the specific antigens in most of them. Celiac shows us the model. The question is whether the same model applies elsewhere."
Lena, 12 — her mother Katrin, 38, speaking. "Lena had been small and tired for years and we had attributed it to her constitution. She was a quiet child and a light eater. It was only when her teacher mentioned that she seemed to be struggling with concentration — more than the other children — that we took it seriously. Her paediatrician ordered bloods and found her anti-tTG at 180. The biopsy showed Marsh grade 3b villous atrophy. She had been absorbing almost nothing from her meals for years. Within six months of removing gluten, her teacher was asking if we had changed her medication — she thought Lena was on a new ADHD drug. She was not on any drug. She was just finally nourished."
Jorge, 67. He was diagnosed with celiac disease at 67, having had gut symptoms attributed to IBS for over two decades. The diagnosis came when his internist ordered an ANA panel for unrelated joint pain and noticed, while reviewing his chart, that his iron had been persistently low for fifteen years with no documented investigation. The gastroenterology referral found total villous atrophy. He had lived without a diagnosis for more than twenty years — a period during which his bones had been demineralised, his iron stores had been chronically depleted, and a correct explanation for his gut symptoms had existed and been missed.
Astrid, 24. She tested negative for celiac antibodies twice and was told she did not have celiac disease. She did not find out about the IgA deficiency until three years later, when a haematologist, investigating something else, noted that her total IgA was undetectable. Celiac antibody testing relies on IgA; in IgA-deficient patients, the standard test produces a false negative. A repeat biopsy — done because she was IgA-deficient and symptomatic — showed partial villous atrophy. She had been given clear reassurance, twice, that she did not have a condition she had. The test had failed her, not her symptoms.